
Interoception: The Sixth Sense That Shapes Your Sexuality & Emotional Life
We navigate the world through our five familiar senses, sight, sound, touch, taste, and smell, interpreting external stimuli to make sense of our environment. Yet beneath conscious awareness runs a parallel sensory system equally essential to our wellbeing, one that most people never learn to recognise or develop. This is interoception: the perception of signals arising from within the body itself.
While neuroscience has long understood interoception as the brain's mechanism for maintaining homeostasis, regulating heart rate, blood pressure, temperature, and other vital functions, emerging research reveals something far more profound. Interoception shapes our emotional landscape, influences our decision-making, determines the quality of our relationships, and fundamentally structures our sense of self.
In the realm of sexuality and intimate connection, interoception becomes even more critical. The capacity to sense and interpret our body's internal signals, arousal, pleasure, discomfort, desire, forms the foundation of authentic sexual expression. Without this internal compass, we drift into performative sexuality, disconnected from our genuine experience and unable to communicate our true needs to partners.
What Is Interoception? The Science of Sensing from Within
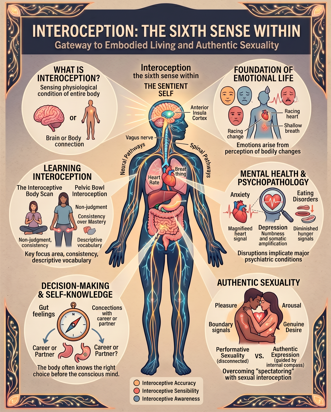
Interoception refers to the perception and integration of signals originating inside the body. Neuroscientist A.D. Craig defines it as "the sense of the physiological condition of the entire body." Unlike exteroceptive senses that orient us to the external world, interoception orients us to our internal landscape.
The interoceptive system comprises specialised sensory receptors distributed throughout the body's organs, muscles, connective tissues, and blood vessels. These receptors continuously monitor conditions, including:
- Cardiovascular signals: heart rate, blood pressure, vascular tension
- Respiratory signals: breathing rate, depth, airway resistance
- Gastrointestinal signals: hunger, fullness, nausea, gut motility
- Muscular signals: tension, fatigue, proprioceptive feedback
- Temperature regulation: core temperature, peripheral warmth or coolness
- Pain and inflammation: tissue damage, immune response
- Sexual and reproductive signals: arousal, genital sensation, hormonal fluctuations
These signals travel primarily via the vagus nerve and spinal pathways to the thalamus and ultimately to cortical regions, including the insula, the brain's primary interoceptive processing centre. The insula integrates raw sensory data with emotional, cognitive, and contextual information to generate the subjective experience of our bodily state.
Three Dimensions of Interoceptive Experience
Contemporary research distinguishes between three interrelated facets of interoception:
Interoceptive Accuracy refers to the objective capacity to detect internal bodily signals. This varies considerably between individuals and appears influenced by genetics, early developmental experiences, trauma history, and sustained attention practice.
Interoceptive Sensibility captures the self-reported tendency to notice internal sensations, essentially, how interoceptively aware people believe themselves to be. Interestingly, this often diverges from objective accuracy.
Interoceptive Awareness represents the most sophisticated dimension: metacognitive insight, or the degree to which objective performance aligns with subjective confidence. This capacity proves particularly important for mental health and adaptive functioning.
Why Interoception Matters: From Survival to Thriving
The Foundation of Emotional Life
Perhaps no contemporary finding has more profoundly shifted our understanding of emotion than the recognition that feelings are fundamentally interoceptive phenomena. When we encounter a threat, our body responds before our conscious mind registers danger: heart rate accelerates, muscles tense, breathing shallows, and digestion slows. The brain perceives these interoceptive changes and generates the subjective experience we label "fear."
Research consistently demonstrates that individuals with higher interoceptive accuracy report more intense emotional experiences and exhibit better emotion recognition in others. People with well-developed interoceptive awareness can differentiate subtle emotional states, distinguishing anxiety from excitement, frustration from disappointment, loneliness from boredom - because they perceive the distinct bodily signatures of each state.
Mental Health and Psychopathology
Disruptions in interoceptive processing implicate virtually every major psychiatric condition, including anxiety disorders, eating disorders, depression, post-traumatic stress disorder, and borderline personality disorder.
In panic disorder, individuals demonstrate heightened interoceptive accuracy for cardiac signals, paired with catastrophic misinterpretation of normal bodily fluctuations. In alexithymia, individuals show markedly reduced interoceptive accuracy, struggling to detect even pronounced bodily changes. Eating disorders present another striking example: individuals with anorexia nervosa demonstrate impaired gastric interoception, diminished capacity to sense hunger and fullness signals, alongside distorted body image.
Decision-Making and Self-Knowledge
Beyond emotion and mental health, interoception fundamentally shapes how we make decisions and know ourselves. Research demonstrates that our bodies often know the right choice before our conscious minds do. When we say something "feels right" or "doesn't sit well," we're literally describing interoceptive sensations. People with higher interoceptive awareness make more advantageous decisions across domains, including financial choices, social judgments, and moral dilemmas.
Interoception in the Sexual Arena
Sexual Arousal as Interoceptive Signal
Sexual arousal is fundamentally an interoceptive phenomenon. The complex cascade of physiological changes comprising arousal, increased blood flow to genitals, heightened skin sensitivity, accelerated heart rate and breathing, muscular tension, all generate interoceptive signals that the brain interprets as desire.
Yet research reveals a troubling disconnect for many individuals between physiological arousal and subjective experience. When individuals cannot accurately perceive or trust their bodily signals, they rely instead on cognitive interpretation, partner expectations, or contextual cues to determine whether they're "actually" aroused. The result: a sexuality divorced from authentic bodily experience.
From Performance to Presence
Diminished interoceptive awareness drives what sex researchers term "spectatoring", the tendency to observe and evaluate one's sexual performance rather than inhabiting sensory experience. During intimate encounters, many individuals report thoughts like "Does this look good? Am I taking too long? Are they getting bored?" These cognitive preoccupations override interoceptive attention.
The antidote lies in cultivating sexual interoception: the capacity to remain oriented toward internal sensations during intimate activity. This involves distinguishing between:
- Pleasure sensations: Where in the body do I feel pleasure? What qualities does it have?
- Arousal states: What is my actual level of arousal versus what I think it should be?
- Boundary signals: What sensations indicate "yes, more" versus "pause" versus "stop"?
- Desire quality: Does this desire originate from my body or from wanting to please my partner?
Communication and Consent
Authentic sexual communication depends on interoceptive literacy. Consider the difference between these two communication styles:
Low interoceptive awareness: "I guess I'm okay with continuing", relying on cognitive assessment rather than bodily sensing.
High interoceptive awareness: "I notice my breathing getting shallow and my belly tensing, which tells me I need to slow down", reporting direct interoceptive observation.
The second style honours bodily wisdom, creating space for genuine negotiation and adjustment. Research confirms this link: individuals with higher interoceptive awareness report clearer sexual boundaries, more authentic desire, higher sexual satisfaction, and greater relationship quality.
Learning Interoception: How to Develop Your Sixth Sense
Unlike the external senses, which develop relatively automatically through exposure, interoception requires intentional cultivation. Fortunately, research demonstrates that interoceptive skills are trainable. Interventions targeting interoceptive awareness, including mindfulness meditation, body scanning, and somatic therapies, produce measurable improvements in interoceptive accuracy, emotional regulation, and mental health outcomes.
Foundational Principles
- Start with what's accessible: Heartbeat and breath are good entry points before progressing to subtler sensations
- Practice non-judgment: The goal is noticing, not changing or evaluating
- Develop descriptive language: Is that sensation tight or constricted? Heavy or dense? Sharp or diffuse? Warm or cool?
- Distinguish sensation from interpretation: "My chest feels tight" is a sensory observation; "I'm anxious" is an interpretation
- Consistency over intensity: Five minutes daily builds skill more reliably than occasional hour-long sessions
Practice One: The Interoceptive Body Scan
Duration: 10–15 minutes | Frequency: Daily or 5 times weekly
Lie comfortably on your back or sit upright with feet grounded. Close your eyes or soften your gaze downward. Without changing your breathing, simply notice its natural rhythm.
Move attention slowly through the body, feet and toes, ankles and calves, knees and thighs, pelvis and buttocks, lower belly, middle torso, chest and heart, shoulders and upper back, arms and hands, neck and throat, face and head.
For each area, ask: What sensations am I noticing? Where exactly is the sensation located? What is its quality, sharp or dull, constant or fluctuating, pleasant or unpleasant? Is there movement in this area, or does it feel static?
When you encounter areas of tension, numbness, or discomfort, resist the urge to immediately change them. Simply notice and describe. After practice, spend 2–3 minutes noting what you discovered.
Practice Two: Pelvic Bowl Interoception and Sacral Awakening
Duration: 15–20 minutes | Frequency: 3–5 times weekly
The pelvis houses our sexual and creative organs, our instinctual impulses, and what somatic psychologists describe as first-chakra energies of survival, safety, and embodied presence. Many people carry trauma, shame, disconnection, or chronic tension in this region. Developing an interoceptive relationship with the pelvic bowl is fundamental to reclaiming embodied sexuality.
Lie on your back with knees bent and feet flat on the floor, hip-width apart. Place your hands on your lower belly, just above the pubic bone.
Begin breathing into your lower belly and pelvis. Notice how the pelvic floor gently descends on inhalation and naturally lifts on exhalation. Continue for 2–3 minutes, simply feeling this natural rhythm.
Mentally trace the pelvic floor's diamond shape: front (pubic bone), back (coccyx), left and right (sitting bones). Without engaging muscles, simply notice sensations in this area: temperature, density, aliveness, numbness, vibration.
Very gently engage the pelvic floor muscles as if stopping the flow of urine (20% effort, not full contraction). Hold for 3 seconds while maintaining steady breathing. Release completely and notice what release feels like. Repeat 5 times, emphasising awareness of the release phase more than engagement.
Shift attention to the sacrum, the triangular bone at the base of your spine. Notice its weight against the floor. Some people sense warmth, heaviness, tingling, or pulsing; others initially sense nothing, which is equally valid.
Before ending, notice your overall state. When ready, stretch gently, roll to one side, and slowly return to sitting.
Important: This practice may bring up emotions or sensations related to sexuality, trauma, or body shame. If overwhelming, open your eyes, ground yourself, and work with a trauma-informed somatic practitioner if needed.
Conclusion: Coming Home to Yourself
Interoception represents far more than a neurological curiosity. It is the foundational sense through which we know ourselves, navigate our inner landscape, and make contact with our essential nature. To develop interoceptive awareness is to come home to the body after a long exile in the realm of thought and external validation.
In a culture that privileges cognitive knowing and external achievement over authentic being, reclaiming interoceptive capacity is a quiet act of reclamation. It means trusting that your body holds wisdom worth listening to, that the felt sense arising from within carries valuable information about how to live.
We are not primarily thinking beings who happen to have bodies. We are fundamentally embodied creatures whose thoughts arise from and remain embedded in somatic experience. The path back to wholeness, to authentic sexuality, to creative aliveness runs directly through the body's internal landscape. Interoception is the sense that makes this return possible.
References
Bechara, A., Damasio, H., Tranel, D., & Damasio, A. R. (1997). Deciding advantageously before knowing the advantageous strategy. Science, 275(5304), 1293-1295.
Chivers, M. L., Seto, M. C., Lalumière, M. L., Laan, E., & Grimbos, T. (2010). Agreement of self-reported and genital measures of sexual arousal in men and women: A meta-analysis. Archives of Sexual Behavior, 39(1), 5-56.
Craig, A. D. (2002). How do you feel? Interoception: the sense of the physiological condition of the body. Nature Reviews Neuroscience, 3(8), 655-666.
Craig, A. D. (2009). How do you feel — now? The anterior insula and human awareness. Nature Reviews Neuroscience, 10(1), 59-70.
Critchley, H. D., & Garfinkel, S. N. (2017). Interoception and emotion. Current Opinion in Psychology, 17, 7-14.
Damasio, A. R. (1994). Descartes' error: Emotion, reason, and the human brain. Putnam.
Damasio, A. R. (1999). The feeling of what happens: Body and emotion in the making of consciousness. Harcourt.
Dunn, B. D., Galton, H. C., Morgan, R., Evans, D., Oliver, C., Meyer, M., & Dalgleish, T. (2010). Listening to your heart: How interoception shapes emotion experience and intuitive decision making. Psychological Science, 21(12), 1835-1844.
Ehlers, A., & Breuer, P. (1992). Increased cardiac awareness in panic disorder. Journal of Abnormal Psychology, 101(3), 371-382.
Farb, N., Daubenmier, J., Price, C. J., Gard, T., Kerr, C., Dunn, B. D., & Mehling, W. E. (2015). Interoception, contemplative practice, and health. Frontiers in Psychology, 6, 763.
Füstös, J., Gramann, K., Herbert, B. M., & Pollatos, O. (2013). On the embodiment of emotion regulation: Interoceptive awareness facilitates reappraisal. Social Cognitive and Affective Neuroscience, 8(8), 911-917.
Garfinkel, S. N., Seth, A. K., Barrett, A. B., Suzuki, K., & Critchley, H. D. (2015). Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biological Psychology, 104, 65-74.
Handy, A. B., & Meston, C. M. (2016). Interoceptive awareness moderates the relationship between perceived partner responsiveness and female sexual functioning. Journal of Sexual Medicine, 13(9), 1369-1377.
Harshaw, C. (2015). Interoceptive dysfunction: Toward an integrated framework for understanding somatic and affective disturbance in depression. Psychological Bulletin, 141(2), 311-363.
Khalsa, S. S., Adolphs, R., Cameron, O. G., Critchley, H. D., Davenport, P. W., & Paulus, M. P. (2018). Interoception and mental health: A roadmap. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 3(6), 501-513.
Khalsa, S. S., Craske, M. G., Li, W., Vangala, S., Strober, M., & Feusner, J. D. (2015). Altered interoceptive awareness in anorexia nervosa. International Journal of Eating Disorders, 48(7), 889-897.
Masters, W. H., & Johnson, V. E. (1970). Human sexual inadequacy. Little, Brown.
Murphy, J., Brewer, R., Catmur, C., & Bird, G. (2018). Interoception and psychopathology: A developmental neuroscience perspective. Developmental Cognitive Neuroscience, 23, 45-56.
Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the body: A sensorimotor approach to psychotherapy. W. W. Norton & Company.
Pollatos, O., Gramann, K., & Schandry, R. (2007). Neural systems connecting interoceptive awareness and feelings. Human Brain Mapping, 28(1), 9-18.
Robson, D. (2021). Interoception: the hidden sense that shapes wellbeing. The Guardian.
If this resonates with you - join Fiona for a 20-minute connection call
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.
